 |
|
April 1999 • Volume 15 • Number 3
Vladimir Martinek, M.D.
[MEDLINE LOOKUP]
Niklaus F. Friederich, M.D., Ph.D. [MEDLINE LOOKUP]
Sections
| Abstract | TOP |
Summary: We report a case of an osteolytic tibial enlargement in association with a pretibial cyst formation 8 months after successful anterior cruciate ligament reconstruction with autologous bone–patellar tendon–bone graft and tibial graft fixation with a bioabsorbable interference screw. No joint inflammatory reaction or graft insufficiency was detected. The patient underwent cyst excision and curettage of the tibial tunnel with full recovery and return to preinjury level of activity 2 months after the revision surgery. To our knowledge, the reported complication is the first obvious adverse reaction to a poly-D,L-lactide interference screw in anterior cruciate ligament surgery.
| Key Words: Anterior
cruciate ligament, Reconstruction,
Bioabsorbable
interference screw, Cyst,
Complication. |
Interference screws have become a popular fixation method in anterior cruciate ligament
(ACL) reconstruction with bone–patellar tendon–bone (BPTB) grafts. Using the
original metal interference screws, some complications were reported in initial and
revision surgeries.1-3
Bioabsorbable interference screws have been hypothesized to eliminate some disadvantages
of metal screws and to improve the postoperative graft imaging.4-6 New types of polymer materials have been developed
in recent years to avoid adverse reactions that were seen after internal fixation of
intra-articular fractures or shoulder stabilization with absorbable fixation device.2,5,7-9 To date, no serious adverse reactions in the knee
have been reported using the new generation of poly-d,L-lactide bioabsorbable interference
screws for graft fixation in ACL reconstruction.2,10
We present a case of ACL reconstruction with autologous BPTB graft and bioabsorbable
interference screw fixation in which an osteolytic cyst formation in the osseous tibial
tunnel, communicating with a symptomatic pretibial cyst at the tibial tunnel aperture, was
noted. To our knowledge, this is the first reported complication in association with a
poly-D,L-lactide interference screw in the knee joint.
| CASE REPORT | TOP |
A 32-year-old man sustained an isolated ACL disruption of his left knee while playing
soccer. Postprimary arthroscopic ACL reconstruction with autologous BPTB using a
2-incision press fit technique (Burkart P, personal communication, 1995) was performed
because of significant instability with grade 3 positive Lachman test and grade 2 positive
pivot shift. In this technique, the BPTB graft was introduced through the proximal conical
formed femoral tunnel, in which the proximal equally conical formed bone block was press
fitted and blocked. The distal bone block fixation was done with a 6 × 23 mm
bioabsorbable interference screw, made of poly-D,L-lactide (Sysorb; Sulzer Orthopedics,
Baar, Switzerland). The patient subsequently did well and returned after 6 months to the
same level of activity as before the injury.
Eight months after the operation, however, the patient noted swelling and pain over the
anterior proximal tibia. There was no history of a new trauma or of a giving way. A
tender, fluctuant mass was palpable over the end of the tibial tunnel and the whole
anteromedial proximal tibia showed inflammatory signs. Radiographs revealed a large
osteolytic formation at the proximal tibial tunnel (Fig 1).
| Figure 1. Anteroposterior radiograph of the left
knee showing a large osteolytic formation at the proximal tibial tunnel 1 year after ACL
reconstruction with BPTB and tibial fixation with bioabsorbable interference screw. |
Click on Image to view full size |
Magnetic resonance imaging showed enlargement of the tibial tunnel, which was filled with fluid and communicated with another pretibial subcutaneous fluid-filled cyst (Fig 2).
| Figure 2. Sagittal magnetic resonance
image showing fluid in the tibial tunnel and extending out of the tibial tunnel forming a
subcutaneous cyst. |
 |
Click on Image to view full size |
The distal bone block of the BPTB graft was integrated in the surrounding bone and the
bioabsorbable interference screw could not be identified. There were no signs of effusion
or synovial hypertrophy within the knee joint. Examination under anaesthesia revealed only
grade 1 Lachman test and negative pivot shift results.
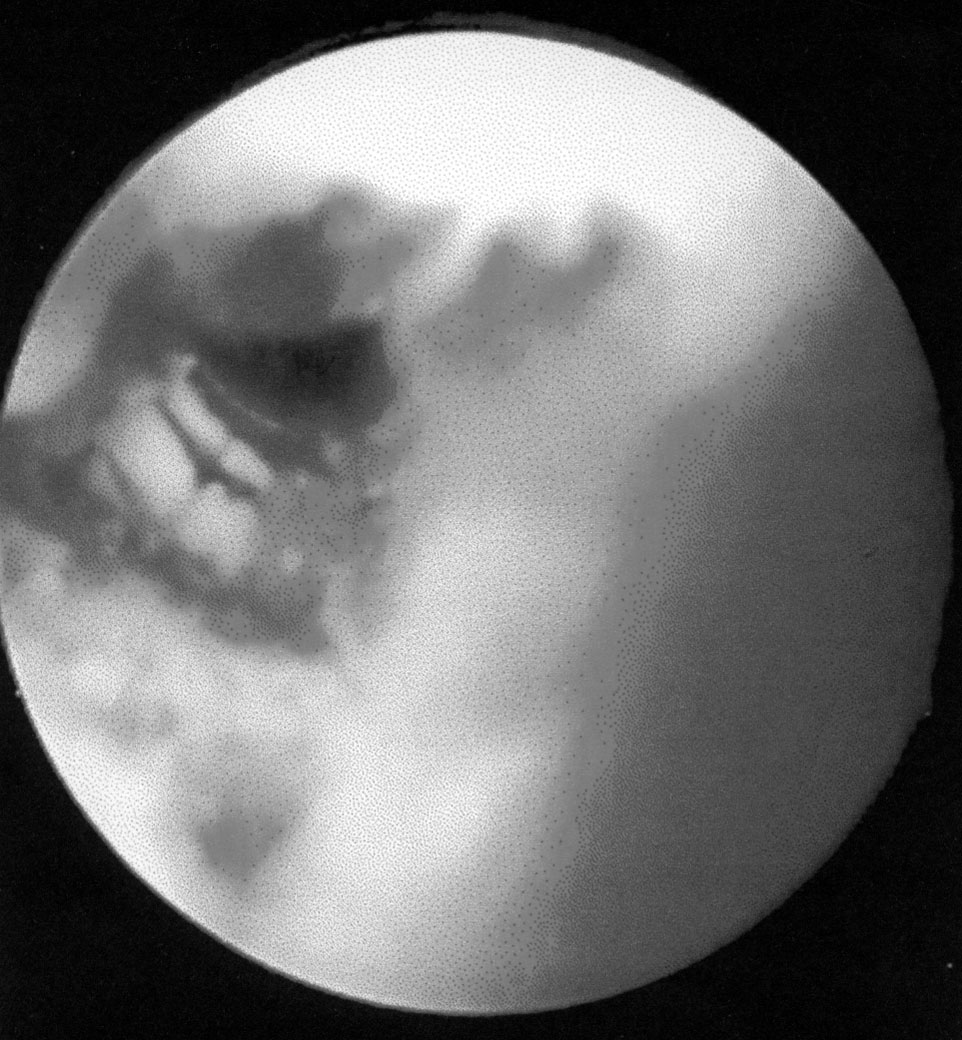
At arthroscopy, the knee joint showed no signs of any intra-articular inflammatory
reaction or foreign body evidence. The ACL graft was intact, covered with normal synovia
(Fig 3), and manifested a good tension at the arthroscopic-controlled Lachman test.
| Figure 3. Arthroscopic view of the
intact ACL graft without any inflammatory reaction inside the knee joint. |
 |
Click on Image to view full size |
Histological examination from the tibial attachment of the ACL did not show any
inflammatory or granulomatous reaction.
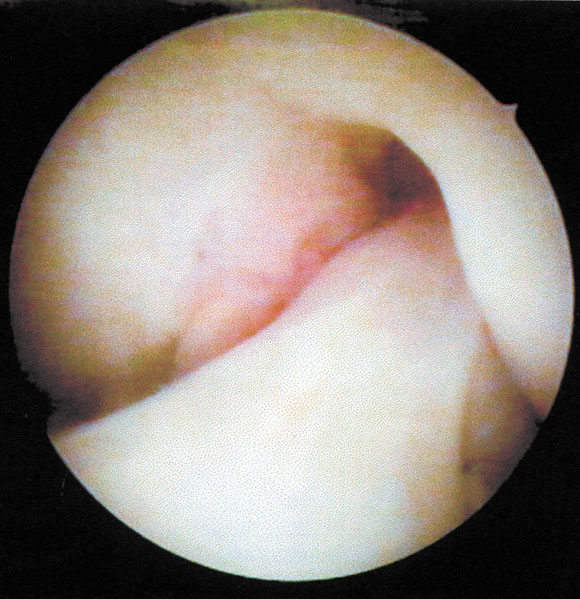
After open excision of the pretibial cyst, which entered directly into the tibial tunnel,
the tunnel was debrided. Inside the tunnel, a remaining part of the head of the
bioabsorbable interference screw was found distally (Fig 4) and, proximally, some cystic
formation was found inside the bone, filled with a gelatine-like mass.
| Figure 4. Arthroscopic view of tibial
tunnel showing the remaining head of the bioabsorbable interference screw beside the
integrated bone block of the graft. |
 |
Click on Image to view full size |
There was no connection between the tunnel cavity and the knee joint. Bone grafting was
not performed. The histological examination of the cyst wall and the gelatine-like mass
did not show any refractile material or inflammatory response. At follow-up 2 months
later, the patient was free of symptoms and there was no evidence of recurrence.
| DISCUSSION | TOP |
Bioabsorbable interference screws composed of poly-lactic acid polymers have been used in
ACL surgery for about 5 years with good clinical results.2,5,6,10
It was thought that foreign body as well as giant cell reactions in soft tissue and bone
or synovitis in joints that were described after using polydioxanone, polyglycolide and
lactide-glycolide polymers would be eliminated.7,8,11 Recently,
however, Takizawa et al.9 reported the case of
a severe gonitis after screw breakage following intercondylar prominence fracture with
poly-L-lactic acid screws. In this case, mechanical irritation of the loosed broken screw
seemed to stimulate the foreign body reaction in the joint. Imhoff et al.6 reported lytic changes around the bioabsorbable PLLA
screws at the femoral site after ACL reconstruction in two female high-level athletes who
underwent very aggressive postoperative rehabilitation.
Subcutaneous pretibial ganglion-like cyst formations similar to the one presented above
were also described after ACL reconstruction with soft-tissue allografts and autografts
using metal hardware for graft fixation.12,13 In these cases, another mechanism was postulated.
Incomplete incorporation of the allograft tissue within the bone tunnels or pressure
necrosis of the graft fibers were proposed as explanation for the cyst development.12,13
In our opinion, the tibial bone tunnel enlargement and the tibial subcutaneous cyst in
this case report were caused by an adverse reaction of the bone to the bioabsorbable
material used. In this case, no substitution of the polymer material took place by osseous
neoformation in the tibial tunnel up to 8 months after the ACL reconstruction. ACL
reconstruction with autologous BPTB using the press fit technique and distal bone block
fixation with the Sysorb bioabsorbable interference screw have been performed in 25
patients among 250 treated with ACL insufficiency since 1996 in our department. The
incidence reported here is the first complication involving bioabsorbable screw fixation,
resulting in a complication rate of 4% in our series.
We believe that the surgeon should be aware of and be prepared to treat this type of
complication. Future clinical studies will show if the advantages of bioabsorbable screws
in ACL surgery prevail over their potential complications.
REFERENCES
![]()
1. Kurosaka M, Yoshiya S, Andrish JT. A
biomechanical comparison of different surgical techniques of graft fixation in anterior
cruciate ligament reconstruction. Am J Sports Med 1987;15:225-229. [MEDLINE]
![]()
2. Bach BR. Potential pitfalls of Kurosaka
screw interference fixation for ACL surgery. Am J Knee Surg 1985;2:76-78.
![]()
3. Kurzweil PR, Frogameni AD, Jackson DW.
Tibial interference screw removal following anterior cruciate ligament reconstruction. Arthroscopy
1995;11:289-291. [MEDLINE]
![]()
4. Barber FA, Elrod BF, McGuire DA, Paulos LE.
Preliminary results of an absorbable interference screw. Arthroscopy
1995;11:537-548. [MEDLINE]
![]()
5. Stähelin AC, Weiler A, Rüfenacht H,
Hoffmann R, Geissmann A, Feinstein R. Clinical degradation and biocompatibility of
different bioabsorbable interference screws: A report of six cases. Arthroscopy
1997;13:238-244. [MEDLINE]
![]()
6. Imhoff AB, Martinek V, Schwamborn T, Merl T.
Bioabsorbable interference screws in ACL reconstruction: A prospective clinical and MRI
study. Oral presentation, 1. European Society of Sports Traumatology, Knee Surgery, and
Arthroscopy Nice, France, April-May 1998.
![]()
7. Bostman OM. Osteolytic changes accompanying
degradation of absorbable fracture fixation implants. J Bone Joint Surg Br
1991;73:679-682. [MEDLINE]
![]()
8. Edwards DJ, Hoy G, Saies A, Hayes MG.
Adverse reactions to an absorbable shoulder fixation device. J Shoulder Elbow Surg 1994;3:230-233.
![]()
9. Takizawa T, Akizuki S, Hiriuchi H, Yasukawa
Y. Foreign body gonitis caused by a broken poly-L-lactid acid screw. Arthroscopy
1998;14:329-330. [MEDLINE]
![]()
10. Stähelin AC, Feinstein R, Friederich NF:
Clinical experience using a bioabsorbable interference screw for ACL reconstruction. Orthop
Trans 1995;19,2:287-288.
![]()
11. Friden T, Rydholm U. Severe aseptic
synovitis of the knee after biodegradable internal fixation. Acta Orthop Scand
1992;63: 94-97. [MEDLINE]
![]()
12. Victoroff BN, Paulos LE, Beck C,
Goodfellow DB. Subcutaneous cyst formation associated with anterior cruciate ligament
allografts: A report of four cases and literature review. Arthroscopy
1995;11:486-494. [MEDLINE]
![]()
13. Simonian PT, Wickiewicz TL, O'Brien SJ,
Dines JS, Schatz JA, Warren RF. Pretibial cyst formation after anterior cruciate ligament
surgery with soft tissue autografts. Arthroscopy 1998;14:215-220. [MEDLINE]
| Publishing and Reprint Information | TOP |